
More Information
Submitted: November 15, 2024 | Approved: November 22, 2024 | Published: November 25, 2024
How to cite this article: Bobokhojaev OI, Abdulloev NN, Khushvakhtov ShD, Shukurov SG. Efficiency of Artificial Intelligence for Interpretation of Chest Radiograms in the Republic of Tajikistan. J Pulmonol Respir Res. 2024; 8(2): 069-073. Available from: https://dx.doi.org/10.29328/journal.jprr.1001064
DOI: 10.29328/journal.jprr.1001064
Copyright License: © 2024 Bobokhojaev OI, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Interpretation of X-ray images; Artificial intelligence; Lung diseases

Efficiency of Artificial Intelligence for Interpretation of Chest Radiograms in the Republic of Tajikistan
Bobokhojaev OI1* , Abdulloev NN2, Khushvakhtov ShD1 and Shukurov SG1
, Abdulloev NN2, Khushvakhtov ShD1 and Shukurov SG1
1State Educational Institution, “Avicenna Tajik State Medical University”, Tajikistan
2Lautoka Hospital, FijiState Educational Institution, “Khatlon State Medical University”, Tajikistan
*Address for Correspondence: Bobokhojaev OI, Professor, Head of the Department of Phthisiopulmonology, State Educational Institution “Avicenna Tajik State Medical University”, Tajikistan, Email: [email protected]
The article presents data from recent publications and own data on screening studies with interpretation of chest radiographs using artificial intelligence CAD (Computer-Assisted Diagnosis), which, according to WHO recommendations, provides more accurate clinical thresholds for deciding who needs to take a sputum test. Another aspect of the WHO recommendations is the cost-effectiveness of CAD as a tool for triaging patients with tuberculosis symptoms in low-income countries with a high incidence of tuberculosis. Compared with smear microscopy and GeneXpert, without preliminary sorting, the use of mobile digital X-ray machines equipped with a CAD tool reduces costs, allowing sorting of individuals suspected of having tuberculosis for testing on GeneXpert, while reducing the time to start tuberculosis treatment.
Thus, conducting a study using portable X-ray machines using a CAD program is a low-cost and easy-to-implement method, does not require large funds, does not require separate rooms, is highly effective, has good image quality, allows you to quickly clarify individuals suspected of having tuberculosis, differentiating it from other pathological changes in the lungs.
Our experience shows that machine analysis of chest computed tomography data, due to the higher resolution capabilities of the method and the absence of fundamental disadvantages of radiography, including the effect of shadow summation, the presence of “blind” zones, etc., is finding increasing application in both diagnostics and screening of respiratory diseases. Our use of this tool allowed us to identify additional new cases of phthisio-onco-pulmonary diseases in field conditions.
According to WHO, the Republic of Tajikistan is among 30 countries in the world with a high burden of tuberculosis, especially its drug-resistant forms. Official statistics on registered cases of tuberculosis differ significantly from WHO estimates on tuberculosis incidence. Thus, if in 2021 WHO estimates indicated an incidence rate of 88 per 100 thousand population (8600 cases), in the country the rate of registered cases in 2021 was only 40.3 per 100 thousand population or 4158 cases [1]. Despite the fact that anti-tuberculosis laboratories in all regions of the country are sufficiently equipped to carry out rapid molecular genetic diagnostics of tuberculosis and its drug-resistant forms (Xpert), the situation with the detection of new cases of the disease, especially after its sharp decline during the COVID-19 pandemic, has not yet reached the pre-COVID level [2,3]. In this regard, the recommendations of the WHO in March 2021 on the active use of innovative approaches based on digital technologies in clinical practice were fully justified. One of these methods is the CAD (computer aid diagnosis) tool installed in portable digital X-ray units [4]. X-ray machines with artificial intelligence also have advantages over conventional chest X-ray examinations in that they can be used by general practitioners who do not have special skills in reading X-ray images, improve the quality of interpretation of chest X-ray images through automation and standardization, have a lower radiation load, reduce the time for interpretation, can provide diagnostics of phthisio-onco-pulmonary diseases and recognize pathologies located in “blind” zones, and allow dynamic comparative monitoring of treatment effectiveness [5]. Of course, CAD cannot replace the comprehensive approach and clinical thinking of a doctor, but it is an effective assistant for a doctor when conducting screening studies [6].
The development of the first artificial intelligence systems for determining lung pathology based on CAD occurred during the COVID-19 pandemic [7]. CAD systems use image pre-processing (increasing contrast, defining lung boundaries, reducing bone structure shadows) to make objects reflecting pathological changes more visible [8]. The complexity of using CAD in screening for pulmonary tuberculosis is directly related to the wide variety of radiographic forms of this disease [9]. Currently, a CAD algorithm has been developed to identify decay cavities on radiographs, which often indicate bacterial excretion in a patient and the risk of severe complications [10]. The development of artificial intelligence in the field of tuberculosis diagnostics has achieved high results, some algorithms are not inferior to the indicators of doctors and can be used for primary reading, but this requires an appropriate regulatory framework and special training [11].
In the CAD literature, two different “use cases” of CXR for TB detection are often mentioned. One is “triage”, where the study population consists of individuals presenting with TB symptoms. The other is “screening”, where the study population is not pre-selected for TB symptoms but is tested because they are at risk for TB [12].
The World Health Organization recommends using Xpert MTB/RIF or sputum culture as the reference standard. However, using sputum alone to diagnose TB often leads to biased estimates due to low sensitivity. This is especially important to consider in settings where the disease is sputum smear-negative, likely in settings with a high prevalence of HIV coinfection [13].
On the other hand, factors such as gender, previous history of TB, age, and HIV status affect the accuracy of CAD. In these cases, the developers recommend calibrating CAD using local data without using reference cutoffs and considering different cutoffs for different populations, especially for people living with HIV. This is one of the major challenges in implementing CAD: developing a program to set the cutoff score in the study before implementation. Without it, interpretation is prone to error, depending on how the study is conducted [14].
A large study has been published comparing commercially available deep learning-based CADs with the GeneXpert sputum microbiology standard in 1,196 symptomatic participants from Nepal and Cameroon. Using GeneXpert as the reference standard, the CAD products had similar performance [15].
In another study, CAD was compared with the performance of a reference standard in two sputum cultures from 2,198 people from an urban tertiary care hospital in Pakistan. In this study, the culture method performed better than CAD [16]. However, in both studies, CAD products outperformed local radiologists when compared with digital radiographs. However, when CAD sensitivity was compared with expert radiologists, the latter had lower specificity than expert radiologists. This highlights the need for rigorous evaluation and independent validation of the performance of all commercial products [17].
Unlike traditional diagnostic tests, new CAD products are frequently introduced and receive regular software releases. CAD products that have been evaluated by WHO and subsequently recommended for use as an alternative to radiograph interpretation have outperformed previous products, demonstrating the need for ongoing re-evaluation and objective re-validation of diagnostic accuracy and threshold calibrations. Currently, WHO is still establishing its prequalification program to adapt to the rapid pace of innovation in this field.
Deep learning algorithms analyzing digital radiographs have also been developed to identify non-TB diseases, including pneumonia, COVID-19, and lung cancer [18]. The results of a comparative analysis of computed tomography (CT) with mobile digital X-ray machines equipped with a CAD tool have been published. It was reported that the CAD reading in the digital X-ray machine correlates better with the radiologist’s readings when interpreting CT [19].
We studied the effectiveness and possibilities of the practical application of artificial intelligence in interpreting radiographs for various phthisio-onco-pulmonological diseases of the lungs. The first digital mobile X-ray units with the installation of the artificial intelligence program CAD (Computer-Aided Diagnosis) were purchased in the Republic of Tajikistan in 2022. Today, trained doctors work on such units in 34 regions of the country. We studied the effectiveness of using these units by carrying out monitoring visits to these regions.
Tajikistan is a country in Central Asia, 93% of whose territory is mountainous, with a population of slightly more than 10 million people, located in the foothills of the Pamirs and bordering Afghanistan, China, Kyrgyzstan and Uzbekistan. In the Republic of Tajikistan, a quarter of the total morbidity is due to respiratory diseases. Over the past decade, the Republic of Tajikistan has recorded an increase in the incidence and mortality rates of respiratory diseases, with various forms with atypical and severe forms of clinical course. As in many countries, respiratory diseases in the republic occupy a leading place in the structure of disability and mortality, depriving a significant part of the population of working capacity, and most often people of mature working age with extensive professional experience and potential for an active life and activity.
In the near future, we plan to connect all CAD XR machines with a single network. This will allow routine collection, storage, and transmission of necessary information on the finding results to the central server. In the meantime, in order to accumulate information, we carry out monitoring visits quarterly.
During 2023, a total of 146,400 CAD studies installed in digital X-ray units were performed, which made it possible to identify 766 additional cases of pulmonary tuberculosis, subsequently confirmed by molecular genetic methods of sputum examination (0.5%). Further microscopic examination of sputum revealed 309 cases of them with bacterial excretion (40.3%). In addition to tuberculosis, we identified 49 new cases of pulmonary echinococcosis, 127 new cases of lung cancer, 244 new cases of pleurisy, and 1222 new cases of other pulmonary diseases (0.8%), which were not previously diagnosed due to the absence of obvious clinical symptoms (Figures 1,2). We (Abdulloev NN) reported this finding results at a recent international scientific conference in Dushanbe [20].
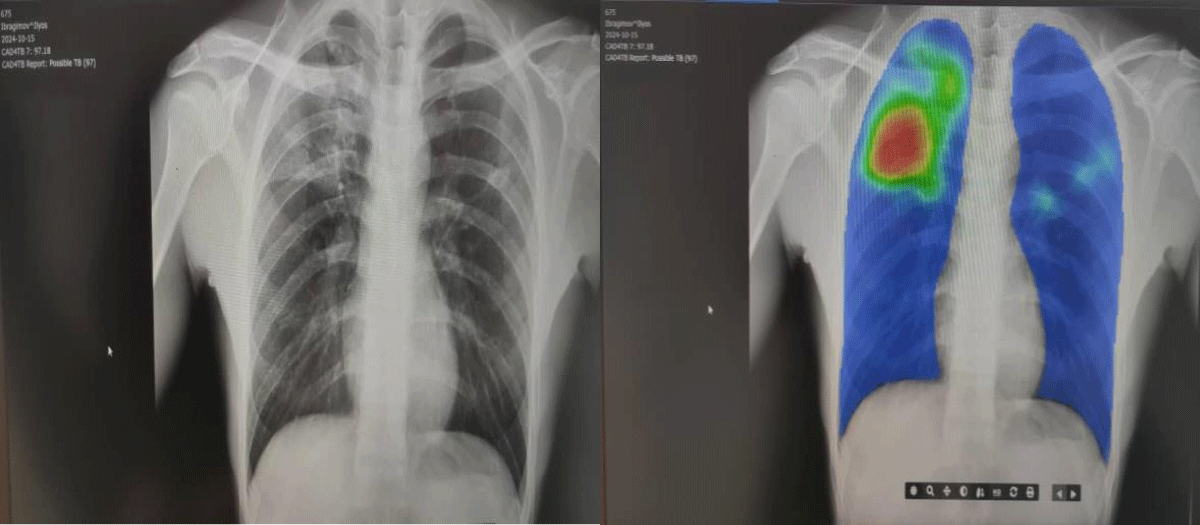
Figure 1: The pictures on the left show a digital chest X-ray of the patient. In the upper left corner, the CAD conclusion about pulmonary TB with a possibility of 97% can be seen. On the right is the CAD interpretation with an overview picture of the same pathological focus.

Figure 2: The two photos above present the CAD in action.
Advantages of CAD: portable in a case, relatively lightweight, generates high-quality images, emits less radiation, and is battery-powered.
The output reports and interfaces of CAD software typically provide [21]:
1. A heat map showing the area of the chest where the lesion is present (“detection”);
2. A numeric lesion score ranging from zero to one (or 0 to 100) for the lesion or disease it can detect (“classification”);
3. A dichotomous (binary) classification of the lesion that the CAD software can detect;
4. An automatically generated standard radiographic report.
5. Provides the ability to improve lesion detection, avoiding inaccuracies in the interpretation of chest radiographs by automating and standardizing the interpretation of radiographic results.
In the context of WHO recommendations for screening with chest radiograph interpretation, CAD provides more accurate clinical cut-off values for deciding who should undergo sputum testing. Another aspect of the WHO recommendations is the cost-effectiveness of CAD as a triage tool for patients with respiratory symptoms in low-income countries with high TB incidence. Compared with smear microscopy and GeneXpert without pre-triage, the use of mobile digital X-ray machines equipped with CAD reduces costs by allowing triage of TB suspects for GeneXpert testing, while reducing the time to initiation of TB treatment. Thus, conducting a study using portable X-ray machines with the use of a CAD program is a low-cost and easy-to-implement method, does not require large funds, does not require separate rooms, is highly effective, has good image quality, allows for rapid clarification of individuals with suspected tuberculosis, differentiating it from other pathological changes in the lungs [22,23].
Although not studied in this paper, the economic efficiency of the widespread implementation of this approach in the country is undeniable. This fact has been confirmed by other studies [12,25-27].
Limitation
Evidence assessing CAD’s diagnostic accuracy is limited by the small number of studies, most of which have important methodological limitations, the availability and evaluation of only one software programme. Additional research is required.
Our experience shows that machine analysis of chest computed tomography data, due to the higher resolution capabilities of the method and the absence of fundamental shortcomings of radiography, including the effect of shadow summation, the presence of “blind” zones, etc., is increasingly used both in the field of diagnostics and screening of lung diseases. Our use of this tool allowed us to identify additional new cases of phthisio-onco-pulmonary diseases in field conditions.
We would recommend that this approach be used more widely in the work of family doctors in general practice, as well as in mass screening for the purpose of preventive examinations of particularly vulnerable populations and during outbreaks of various respiratory diseases.
- World Health Organization. Global TB Report 2022. WHO; 2022. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022
- Bobokhojaev OI. Experience in optimizing the accessibility of services for tuberculosis in the Republic of Tajikistan. J Community Med Health Solut. 2022;3:064-068. Available from: https://doi.org/10.29328/journal.jcmhs.1001022
- Bobokhojaev OI. Long term results of 10 years of observation of cured cases of pulmonary tuberculosis. J Pulmonol Respir Res. 2022;6:007-011. Available from: https://doi.org/10.29328/journal.jprr.1001036
- World Health Organization. Chest radiography in tuberculosis detection – summary of current WHO recommendations and guidance on programmatic approaches. WHO; 2016. Available from: https://www.who.int/publications/i/item/9789241511506
- Adams SJ, Henderson RDE, Yi X, Babyn P. Artificial intelligence solutions for analysis of X-ray images. Can Assoc Radiol J. 2021 Feb;72(1):60-72. Available from: https://doi.org/10.1177/0846537120941671
- Khan AI, Shah JL, Bhat MM. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest x-ray images. Comput Methods Programs Biomed. 2020;196:105581. Available from: https://doi.org/10.1016/j.cmpb.2020.105581
- Apostolopoulos ID, Mpesiana TA. COVID-19: automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys Eng Sci Med. 2020;43:635-640. Available from: https://doi.org/10.1007/s13246-020-00865-4
- Ather S, Kadir T, Gleeson F. Artificial intelligence and radiomics in pulmonary nodule management: current status and future applications. Clin Radiol. 2020;75(1):13-19. Available from: https://doi.org/10.1016/j.crad.2019.04.017
- Behzadi-Khormouji H, Rostami H, Salehi S, Derakhshande-Rishehri T, Masoumi M, Salemi S, et al. Deep learning, reusable and problem-based architectures for detection of consolidation on chest X-ray images. Comput Methods Programs Biomed. 2020;185:105162. Available from: https://doi.org/10.1016/j.cmpb.2019.105162
- Chassagnon G, Vakalopoulou M, Paragios N, Revel MP. Artificial intelligence applications for thoracic imaging. Eur J Radiol. 2020;23:108774. Available from: https://doi.org/10.1016/j.ejrad.2019.108774
- CAD and X-ray training modules. Stop TB Partnership. 2022. Available from: https://www.stoptb.org/resources-implementing-cad-and-xray/cad-and-x-ray-training-modules
- Bashir S, Kik SV, Ruhwald M, Khan A, Tariq M, Hussain H, et al. Economic analysis of different throughput scenarios and implementation strategies of computer-aided detection software as a screening and triage test for pulmonary TB. PLoS One. 2022;17(12):e0277393. Available from: https://doi.org/10.1371/journal.pone.0277393
- Dvijotham KD, Winkens J, Barsbey M, Ghaisas S, Stanforth R, Pawlowski N, et al. Enhancing the reliability and accuracy of AI-enabled diagnosis via complementarity-driven deferral to clinicians. Nat Med. 2023;29(7):1814-1820. Available from: https://doi.org/10.1038/s41591-023-02437-x
- Dohal M, Porvaznik I, Solovic I, Mokry J. Advancing tuberculosis management: the role of predictive, preventive, and personalized medicine. Front Microbiol. 2023;14:1225438. Available from: https://doi.org/10.3389/fmicb.2023.1225438
- Hwang EJ, Goo JM, Nam JG, Park CM, Hong KJ, et al. Conventional versus artificial intelligence-assisted interpretation of chest radiographs in patients with acute respiratory symptoms in the emergency department: A pragmatic randomized clinical trial. Korean J Radiol. 2023;24(3):259-270. Available from: https://doi.org/10.3348/kjr.2022.0651
- Habib SS, Rafiq S, Zaidi SMA, Ferrand RA, Creswell J, Van Ginneken B, et al. Evaluation of computer-aided detection of tuberculosis on chest radiography among people with diabetes in Karachi, Pakistan. Sci Rep. 2020;10:6276. Available from: https://doi.org/10.1038/s41598-020-63084-7
- Katende B, Bresser M, Kamele M, Chere L, Tlahali M, Erhardt RM, et al. Impact of a multi-disease integrated screening and diagnostic model for COVID-19, TB, and HIV in Lesotho. PLOS Glob Public Health. 2023;3(8):e0001488. Available from: https://doi.org/10.1371/journal.pgph.0001488
- Klinkenberg E, Floyd S, Shanaube K, Mureithi L, Gachie T, de Haas P, et al.; TREATS study team. Tuberculosis prevalence after 4 years of population-wide systematic TB symptom screening and universal testing and treatment for HIV in the HPTN 071 (PopART) community-randomized trial in Zambia and South Africa: A cross-sectional survey (TREATS). PLoS Med. 2023;20(9):e1004278. Available from: https://doi.org/10.1371/journal.pmed.1004278
- Qin ZZ, Barrett R, Del Mar Castro M, Zaidi S, Codlin AJ, Creswell J, et al. Early user experience and lessons learned using ultra-portable digital X-ray with computer-aided detection (DXR-CAD) products: A qualitative study from the perspective of healthcare providers. PLoS ONE. 2023;18:e0277843. Available from: https://doi.org/10.1371/journal.pone.0277843
- Abdulloev NN, Rustamzoda ShD, Sattorov BA. Effectiveness of the implementation in the Republic of Tajikistan of a new innovative approach to the use of artificial intelligence for the interpretation of chest radiographs. In: Materials of the scientific and practical conference of the SEI ATSMU "New Horizons in Medical Science, Education, and Practice", with international participation. November 1, 2024;1:226.
- Yang Y, Xia L, Liu P, Yang F, Wu Y, Pan H, et al. A prospective multicenter clinical research study validating the effectiveness and safety of a chest X-ray-based pulmonary tuberculosis screening software JF CXR-1 built on a convolutional neural network algorithm. Front Med (Lausanne). 2023;10:1195451. Available from: https://doi.org/10.3389/fmed.2023.1195451
- Bobokhojaev OI, Rasulov EF, Abdurakhimov AA. Detection of pulmonary tuberculosis in the Republic of Tajikistan. Hospice & Palliative Medicine International Journal. 2024;7(3):96-98.
- Bobokhojaev OI, Pulatova SJ, Saidova SN. Similarities in measures to prevent the spread of COVID-19 and tuberculosis. CME Journal of Clinical Case Report. 2024;1(1):1-3. Available from: https://www.wecmelive.com/open-access/similarities-in-measures-to-prevent-the-spread-of-covid19-and-tuberculosis.pdf
- Pande T, Cohen C, Pai M, Ahmad Khan F. Computer-aided detection of pulmonary tuberculosis on digital chest radiographs: A systematic review. Int J Tuberc Lung Dis. 2016;20(9):1226-30. Available from: https://doi.org/10.5588/ijtld.15.0926
- Santos AdS, de Oliveira RD, Lemos EF, Lima F, Cohen T, Cords O, et al. Yield, efficiency, and costs of mass screening algorithms for tuberculosis in Brazilian prisons. Clin Infect Dis. 2021;72(5):771-7. Available from: https://doi.org/10.1093/cid/ciaa135
- Philipsen R, Sanchez C, Maduskar P, Melendez J, Peters-Bax L, Peter J, et al. Automated chest-radiography as a triage for Xpert testing in resource-constrained settings: A prospective study of diagnostic accuracy and costs. Sci Rep. 2015;5(1):12215. Available from: https://doi.org/10.1038/srep12215
- MacPherson P, Webb EL, Kamchedzera W, Joekes E, Mjoli G, Lalloo DG, et al. Computer-aided X-ray screening for tuberculosis and HIV testing among adults with cough in Malawi (the PROSPECT study): A randomised trial and cost-effectiveness analysis. PLoS Med. 2021;18(9):e1003752. Available from: https://doi.org/10.1371/journal.pmed.1003752